
Brain-controlled exoskeletons for stroke rehabilitation
Technology transfer from prototype to home use
A stroke is one of the most common causes of acquired disability in the world. 17 million people suffer a stroke each year, and it affects the patient and relatives in terms of decreased quality of life and an increased economic burden on the healthcare sector. After the completion of rehabilitation at a rehabilitation clinic, the injury still affects more than 50% of all patients. Therefore, there is a need for new tools to improve the rehabilitation of these patients.
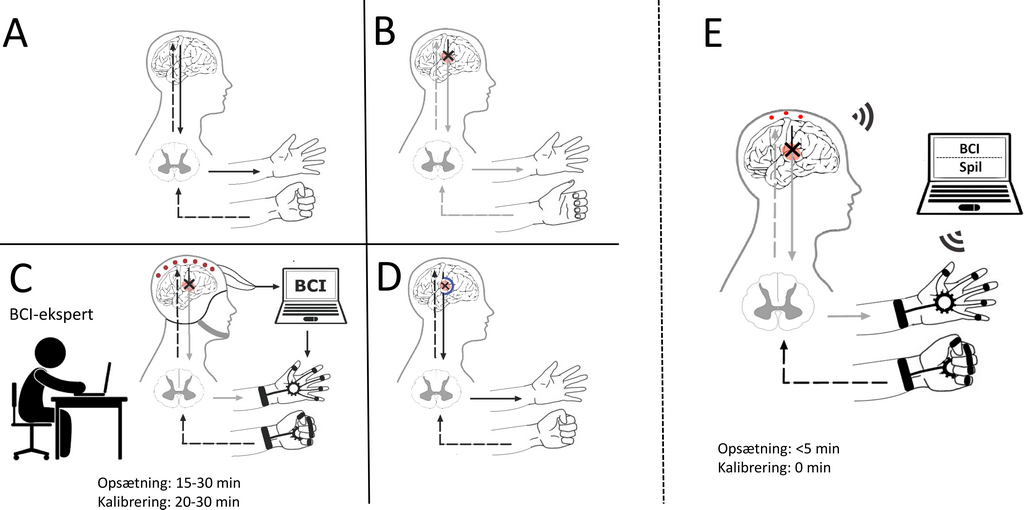
A new promising rehabilitation tool is a brain-controlled exoskeleton (also known as a brain-computer interface) that can help the patient execute the intended movement of the affected limb. This rehabilitation tool is still in the development/evaluation phase. Thus, there is very limited knowledge about how this tool must be designed and implemented, so the patient wants to use it and it is possible to move it out into the rehabilitation clinic or the home of the patient. This will be investigated in a 3-year project supported by VELUX FONDEN with 2.5 million DKK.
The project’s hypotheses are:
- It is possible to create a simple and robust brain-controlled exoskeleton for the hand (a cap and a glove to wear) that can be used by all patients in the hospital, rehabilitation clinic or in their home
- The training with the hand exoskeleton can be adapted to the individual patient and it can be motivating and challenging to use.
The project has technical and clinical aspects, which are tied together by user involvement of patients and those that support the rehabilitation (e.g. relatives and health professionals) in different sectors and regions.
The results can potentially improve the future rehabilitation of a large number of stroke patients in Denmark and in the rest of the world.
The primary investigator is Mads Jochumsen with a collaborative research team consisting of Birthe Dinesen, Hendrik Knoche (Department of Architecture, Design and Media Technology), Troels W. Kjær (Roskilde Hospital, Copenhagen University), and Preben Kidmose (Århus University).